Subscribe!

Hospital Association of Rhode Island (HARI): EDs have become the Front Door of Care
Hospital emergency departments (ED) have become the front door for care
The Hospital Association of Rhode Island says hospital emergency departments have become the front door for medical care, open 24/7, treating every patient who arrives.
They say:
“This is true not only in times of emergencies but also for patients who have lost coverage, can’t access a primary care doctor, or are having a behavioral health crisis. In recent years, emergency departments have increasingly become where the healthcare system’s challenges converge, serving both as critical centers of care and as a reflection of broader system strains.
When patients lose insurance coverage, face high deductibles, or are unable to afford routine care, they frequently delay treatment until their condition worsens, at which point the emergency department remains their only guarantee for care.
Delayed care is typically more complex and costly, increasing the likelihood of hospitals absorbing uncompensated or under-reimbursed care. According to research from the Commonwealth Fund, if people lose Medicaid coverage and become uninsured, hospitals will face a significant increase in uncompensated care expense – from 29.5% to 33.6% – and further strain the stability of our hospitals.
The downstream impacts of these losses affect more than just hospital finances – they cost time and access for all patients and communities.
On top of that, according to the Commonwealth Fund 2025 State Scorecard, Rhode Island has approximately 150 potentially avoidable ED visits per 1,000 employer-insured enrollees aged 18-64 and nearly 133 potentially avoidable ED visits per 1,000 65+ aged Medicare beneficiaries.
More than 21,000 (6.4%) of all emergency department visits in 2022 were considered potentially preventable with timely, accessible outpatient care, according to data from the R.I. Department of Health. Potentially preventable visits to the ED increase wait times and crowding, and strain limited hospital staff resources. These potentially preventable visits alone cost Rhode Islanders as much as $18 million, excluding non-urgent ED visits, which are a distinct and larger category of utilization that would increase those costs.
Coverage instability, limited capacity in other care settings, and gaps in services don’t just make medical needs disappear; instead, they show up in emergency rooms, where care is resource-intensive and poorly suited for routine or ongoing needs.
This is why our hospitals remain committed to working with state leaders, the General Assembly and healthcare partners across the state to alleviate the strains on our EDs and patients. We can address these systemic issues by improving access to primary and behavioral health care, reducing administrative burdens, stabilizing insurance coverage and protecting hospital funding. These solutions are within our grasp and will take ongoing partnership to make possible.”
___
Recognizing the critical time in accessing healthcare that it is, RINewsToday asked HARI to respond to 6 questions:
- What about the huge wait times in hospital emergency departments – with common experiences of sick people waiting for hours in crowded waiting rooms, often right next to others who are visibly ill?
- Women being forced to deliver their babies without epidurals or other invasive pain control methods because a room is not available and they “don’t do that in the ED” – Also, that several maternity hospitals in other states we quickly researched maintain a small “OR” ready room, of sorts, in their EDs just for this purpose – or a special area on the floor where maternity rooms are so specialized anesthesiologists can stay close to all patients.
- Why are emergency room department wait times no longer appear on hospital websites as they once did, so you can know how long wait times are if you are headed to the hospital – you may choose to go to an urgent care center or another hospital?
- PCPs not extending hours extra “winter sick hours” – and routinely advising people to “go to the emergency room” when they call after hours or when appointment times are not available
- Stat orders for simple procedures such as echocardiograms are not available at facilities on weekends or holidays – leaving people being directed to go to their local hospital with the order.
- Finally – a comment about urgent care centers picking up the slack in emergency care – how do hospitals react to that and the trend for hospitals to “own” and open their own urgent care centers, in communities.
___
New Primary Care
As we publish this today, Brown University Health opens a NEW primary care practice in Middletown. Located at 99 East Main Road, Suite 19A, in Middletown. Participating in the event are:
- Babar Khokhar, MD, President, Brown Health Medical Group, EVP and Chief Physician Officer, Brown University Health
- Cindy Peterson, EVP, Ambulatory and Urgent Care, Brown University Health
- Tracey Wallace, SVP Clinical Services, Brown University Health
- Ed McGookin, MD, Chief of Primary Care, Brown Health Medical Group Primary Care
- Chip Malloy, VP Operations, Brown Health Medical Group Primary Care
- Brown Health Medical Group Primary Care directors and practice managers
- Brown Health Medical Group Primary Care, Middletown clinicians, and staff
___
Response from HARI:
The Hospital Association of Rhode Island has been advocating for funding and improvements to Rhode Island’s healthcare system – from primary care reimbursements to stable and reliable funding for hospitals. Decades of underinvestment have led to shortages across healthcare service areas, like emergency rooms, primary care and mental health.
Some of the statements and questions you posed are in reference to issues in other states, while some are outside of the control of hospitals, like PCPs and their hours.
Rhode Island’s healthcare system, like those around the nation, is under real pressure. Hospitals continue to absorb rising costs for labor, supplies, medications and equipment, while payments from insurers and Medicaid continue to fall short of the actual cost to care. At the same time, thousands of Rhode Islanders may lose health coverage, driving more patients to emergency departments without the means to pay. In 2024 alone, Rhode Island hospitals absorbed more than $84 million in uncompensated care. If even a fraction of newly uninsured patients rely on emergency rooms, inpatient units, or outpatient clinics for the care they need, uncompensated care costs will climb sharply, further jeopardizing hospitals’ financial stability and services.
When funding doesn’t keep pace, the consequences are clear: reduced access to care, strained healthcare workers, and weakened services in every corner of our state. When hospitals are under strain, it’s felt throughout the entire system. Patients wait longer or must travel further for care. Nurses, doctors, and other healthcare workers are stretched to their limits. And essential programs are reduced or cut altogether.
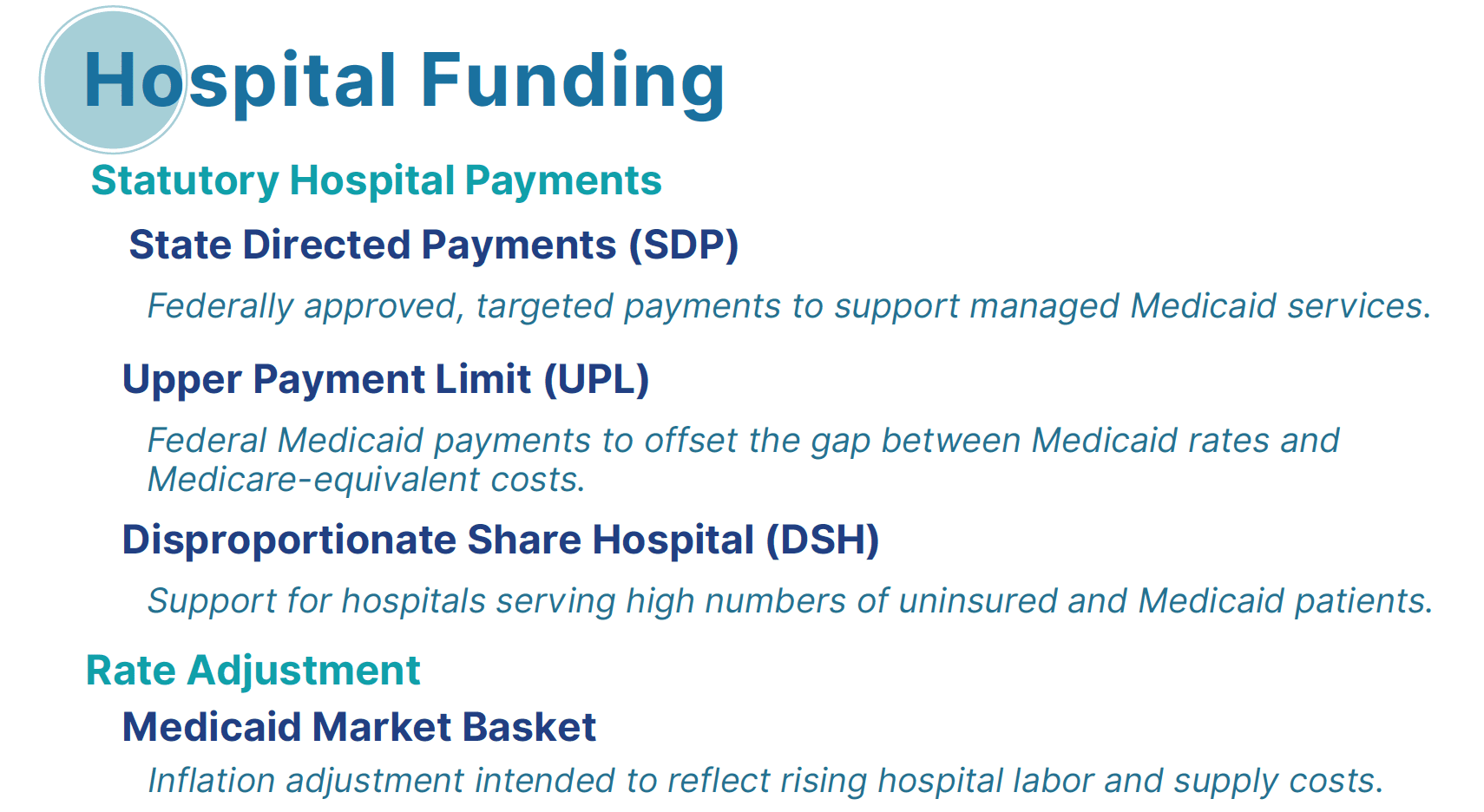
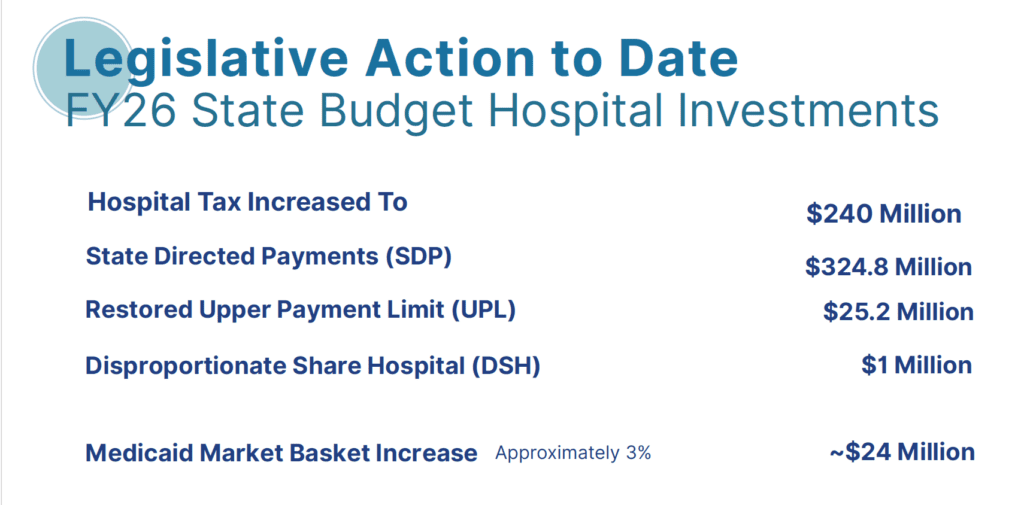
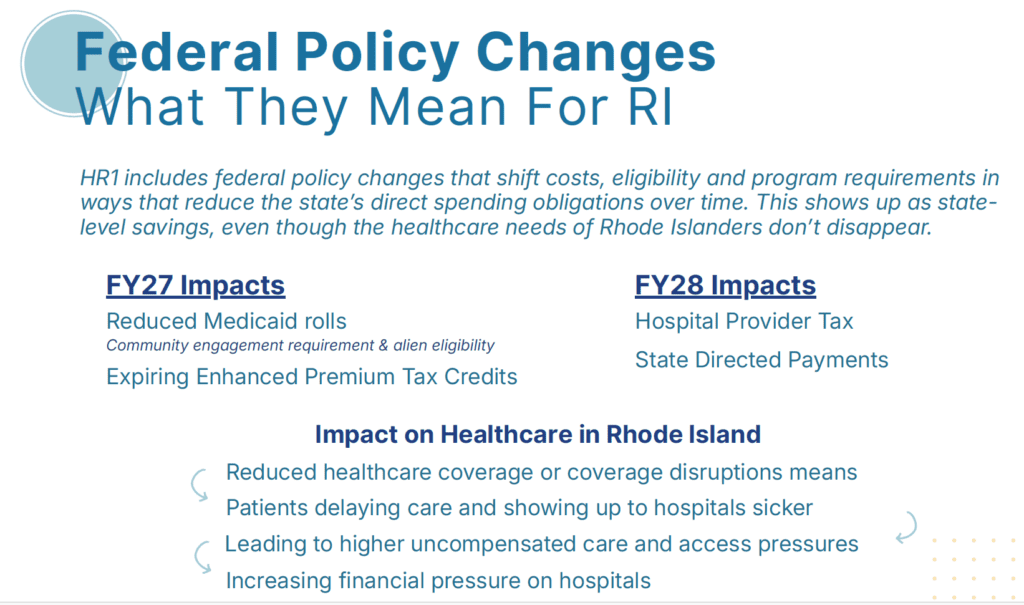
A slide deck from HARI was provided to give additional context as to how we got here, what issues are exacerbating the problem and how the federal changes will impact.
Here is the slide deck:


The disparity in reimbursement for RI physicians, especially those in primary care, is significantly lower than neighboring Connecticut and Massachusetts (and actually lower than most New England states. This serves as the greatest challenge to physician recruitment for RI. Why can’t Medicare address this issue and “even the playing field” ? While there is a nationwide shortage of primary care providers, this fact places RI at a particular disadvantage, one which will not be overcome by simply establishing a new medical school at URI.