Subscribe!

Who Pays When People Without Health Insurance Get Sick?
Even without health insurance, people can get emergency hospital care under federal law in every state. Hospitals are later reimbursed by the government for part of the cost — meaning taxpayers share the expense for care the uninsured receive.
Who Pays When People Without Health Insurance Get Sick? We Do. Taxpayers.
Hospitals must treat everyone, insured or not. Taxpayers already cover more than $150 million a year in Rhode Island for uncompensated care.
The reality today
Many people think that if you don’t have health insurance, you can’t get medical care. That’s not true. By law, every hospital emergency room in the United States must help anyone who is sick or hurt — even if they can’t pay. This law, called EMTALA (the Emergency Medical Treatment and Labor Act), requires hospitals to provide emergency treatment to all.
Afterward, hospitals send bills. Many patients without insurance can’t pay them. Hospitals classify that as uncompensated care — medical care that costs money but goes unpaid.
There are two kinds of unpaid care:
-
Charity care — when hospitals provide free or reduced-cost treatment for low-income patients.
-
Bad debt — when hospitals issue bills that are never paid.
Hospitals don’t simply absorb those losses. The federal government — through Medicare and Medicaid — reimburses hospitals for part of the cost through Disproportionate Share Hospital (DSH) payments. Those funds ultimately come from taxpayer dollars.
So while people without insurance can still receive care, the cost is shared by the public through state and federal support programs.
Rhode Island’s share
Rhode Island hospitals receive more than $140 million annually from a combination of federal and state programs that help offset care for uninsured and low-income patients.
That includes:
-
About $145 million in federal DSH payments.
-
Roughly $20 million in other state Medicaid support.
Hospitals such as Rhode Island Hospital, The Miriam, Roger Williams, and South County Hospital all depend on these funds.
Even with this support, hospitals recover only part of what is owed. The remainder becomes a financial burden that hospitals absorb or shift to other paying patients.
For-profit and nonprofit hospitals
All hospitals — whether for-profit or nonprofit — must provide emergency care under EMTALA. Rhode Island’s hospitals are nonprofit and qualify for larger amounts of federal and state support. When Landmark Medical Center was taken over by PrimeHealthcare, that hospital became the first for profit, but years later they became non-profit, joining the others in the state. When they were for profit, they were also eligible for reimbursement, at different levels.
Important to note is that nonprofit hospitals must document “community benefit” programs to maintain their tax-exempt status. For-profit hospitals, which pay taxes, do not file charity-care reports but remain obligated to provide emergency treatment to everyone who needs it.
Other options for the uninsured – beyond going to the Emergency Room
People without health insurance in Rhode Island aren’t limited to emergency rooms. Several community health centers and free clinics provide basic care regardless of immigration status or income.
Examples include:
-
Rhode Island Free Clinic in Providence — serves uninsured adults statewide.
-
Clinica Esperanza / Hope Clinic — offers care to working people who don’t qualify for other coverage.
These clinics operate outside Medicaid, relying on donations, grants, and volunteer clinicians.
Rhode Island’s Health Equity Zones (HEZs) also play a role — though they do not provide medical care directly, they connect residents to free or low-cost clinics, organize community health screenings, and host wellness programs such as flu clinics and blood-pressure checks across the state.
Still, access is limited, and many uninsured adults continue to rely on emergency rooms as their only point of entry into the health-care system.
The bottom line
People without health insurance can still get emergency care.
Hospitals are required by law to treat them.
Hospitals recover part of those costs through taxpayer-funded programs — and the rest through higher prices or losses.
In Rhode Island, that help adds up to well over $150 million a year.
What could change next – and what is “page 57”?
A new federal proposal could change how that system works, especially for people in other states that do not have the medical treatment available that we do in Rhode Island.
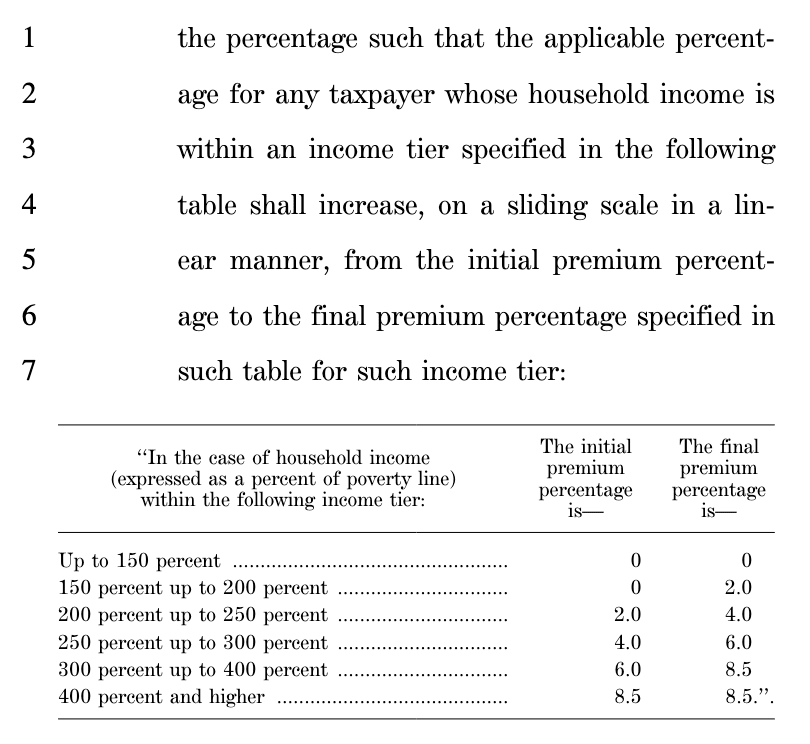
Buried in the Democrats’ FY 26 Continuing Resolution, on page 57, is a single sentence that forbids using Medicaid funds for individuals “not lawfully present in the United States.” Democrats are now proposing to repeal that language which would expand Medicaid for their use in the hospital setting, but also outside of that setting, including doctors’ offices and clinics.
“None of the funds made available under this Act may be used to provide Medicaid, Medicaid-related activities, or other health services under the Medicaid program to individuals who are not lawfully present in the United States.”
FY 26 Democratic Continuing Resolution — page 57:
Other Health Insurance Issues
ACA premium subsidies are a core fight. The shutdown standoff is centered on whether to extend the enhanced ACA premium tax credits before Open Enrollment (starts Nov 1); letting them lapse would raise premiums for millions.
What isn’t impacted right now (or minimally) – for Rhode Islanders
-
Rhode Island’s EOHHS says Medicaid benefits are being processed normally and “the federal government shutdown has not impacted our services to Rhode Islanders at this time.” eohhs.ri.gov
-
Similarly, the state’s DHS pages (for assistance programs) note “no impact on services — all benefits are being processed as usual.” RI DHHS
-
HealthSource RI already is sounding alarms over federal subsidy policy changes, but in practice current enrollees are continuing coverage under existing rules until those policies change. healthsourceri.com
The real risk looms for 2026: roughly 40,000 Rhode Islanders who depend on enhanced ACA premium tax credits face major affordability shocks if Congress allows those credits to expire. Insurers are already requesting double-digit rate increases in anticipation. RI is watching whether the state will try to plug gaps or expand its own subsidy efforts.
So bottom line: day-to-day operations for Medicaid, state assistance, and marketplace enrollment are continuing—for now.
___
Rhode Island Government – Health Access Watch
Brown Health merger aims to expand care to 40,000 more patients — but questions remain
When Attorney General Peter Neronha approved Brown Health’s merger of its two main physician groups — Brown Physicians, Inc. and Coastal Medical — he required the organization to dramatically increase primary care access. Under the agreement, Brown Health must expand capacity to serve up to 40,000 additional Rhode Islanders who currently lack a primary care doctor.
The commitment doesn’t mean 40,000 new patients will appear overnight. Instead, Brown Health plans to combine administrative systems, share clinicians, and streamline operations so more people can be seen through existing practices. The merger allows for expanded use of nurse practitioners, physician assistants, and team-based care, freeing doctors to take on more patients.
Rhode Island faces one of the most acute shortages of primary care physicians in New England. The Attorney General’s office says this merger was approved only with “conditions ensuring measurable community benefit.” Brown Health must report regularly on access growth, and failure to meet targets could trigger additional state action.
Critics, meanwhile, question whether merging two existing networks will truly translate into more exam rooms and appointments — or just larger corporate integration. Supporters argue that, if managed well, the consolidation could reduce wait times, reopen closed patient panels, and expand care in underserved communities.
AI assisted with photo, some data
Excellent resource. Thank you